
No matter how much you know about medicine and anesthesiology, you’re going to come face-to-face with cases that challenge you. Whether it’s the patient’s disease process, their overall health status, or considerations stemming from the surgical procedure itself, some cases are going to present a challenge. And when those factors all combine with patient beliefs that prevent you from using some of your most important tools, you just set up for the case and know that you’re screwed six ways to Sunday.
My patient was a 33-year-old black woman with Marfan syndrome. She had suffered an ascending aortic aneurysm with subsequent dissection. Her chart showed that she had presented to an emergency room two months prior for chest pain, but a full workup had been unrevealing. At the time of her dissection, she had become neurologically compromised, and on the day of her surgery she was in the ICU intubated but requiring no sedation. She had also become hemodynamically unstable and her kidneys had failed; she was on CRRT. She had anasarca with her tongue so swollen that it protruded several centimeters from her mouth; it was obvious that if we dislodged her endotracheal tube she would asphyxiate as we were unlikely to be able to replace it. Similarly, we could see that placement of her lines was going to be very complicated.
The surgical plan was, of course, for median sternotomy, cardiopulmonary bypass, and repair of her dissected aneurysm. Bypass causes notable dilution of the patient's blood, and transfusion of red blood cells and other blood products is very common in such cases. This patient, starting with her hemoglobin a very anemic 7.3 gm/dL, would certainly require transfusion.
Except that she was a Jehovah's Witness.
It's not much fun to walk into a case knowing that your patient will die if she doesn't have surgery, but that she'll probably die because of the surgery. The only solace you can take is from the knowledge that no matter what you do, it's going to be very difficult for you to make her any worse. Some consolation.
The procedure and anesthetic management had been discussed at length with the patient's family, and their wishes had been made extremely clear. We documented everything imaginable, partly so we could honor the patient's and the family's wishes and partly so we would know what fluids we would be able to administer. The patient could receive no red blood cells, platelets, or plasma, but she could receive albumin, recombinant factor VII, and Cell Saver.
My attending and I made the best of it and prepared for the procedure. He handled transport since my mobility is still limited by my tibial fracture. The anesthesia techs helped with positioning and monitoring the patient, and I scrubbed and gowned for the placement of lines.
This patient already had a triple-lumen central line in her left IJ and it was simple to swap it over a wire for one of the double-lumen lines preferred at this particular hospital. Placement of a MAC in her right IJ was a bit more complicated due to her extreme edema. With virtually no neck mobility and great difficulty in retracting her edematous folds of skin, a two-handed procedure became a four-handed one as my attending and I each retracted skin in opposite directions, he handled the ultrasound, and I drove the needle. We ultimately prevailed, though, and the case was soon underway.
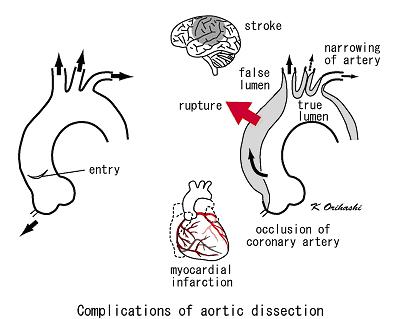
Transesophageal echocardiography is a very useful tool in assessing the anatomy and function of the heart and the great vessels. This young lady's TEE was wretched. It showed a functional heart pumping blood into a badly traumatized aorta, a massive communication evident whereby blood could move from the true lumen to the pseudolumen. The pseudolumen had grown in size until it dwarfed the true lumen; I thought it miraculous that the patient still had peripheral pulses. The surgeons and my attending, for whom cardiac surgery and cardiac anesthesia are daily aspects of life, seemed impressed by the extent of her dissection.
For several hours, the surgeons worked, opening the young woman's chest and repairing her aorta. All along, there were indications of how sick this young woman truly was. Her BIS was constantly low, starting in the mid-20s when we rolled into the room and actually going to 00 with a flat EEG on 0.3 MAC of isoflurane, indicating the probable extent of her neurological devastation. We drew no unnecessary lab work, regarding every milliliter of her blood as a precious commodity that should not be wasted. An ABG drawn shortly after initiation of bypass showed that she was severely anemic, with a hemoglobin concentration of about 6 gm/dL. Instead of waiting until the end of the case to administer Cell Saver blood, we asked the perfusionist to start making whole and half units as soon as he was able.
And still the surgeons worked. They were ultimately successful in repairing her aorta, and we all breathed sighs of relief as the patient tolerated the weaning of cardiopulmonary bypass with only two vasoactive infusions. The sternotomy was closed and the attending surgeon scrubbed out to dictate the case as his assistant continued with skin closure.
But as he closed, the patient began to deteriorate. Her pressures worsened, her heart rate accelerated, and her BIS, already tenuous, dropped. Fearing what we would see, my attending and I looked at the TEE and found the diagnosis: cardiac tamponade. The patient was bleeding into her pericardial sac, and the blood looked like it was already clotting.
We showed the junior surgeon what we had seen and he immediately began cutting the sutures holding the patient's chest closed. The attending surgeon hastily scrubbed back into the case and within a minute the patient's sternotomy had been reopened. My attending and I watched the surgeons scoop clotted blood from the patient's pericardium, knowing that every red blood cell lost to that clot was a cell she needed desperately.
As the surgeons closed the patient's chest again, we very cautiously administered albumin to maintain a reasonable blood volume without hemodiluting the patient too much. By the end of the case, the patient's total fluid input was just one liter of albumin and 300 ml of lactated Ringers. And still her final hemoglobin was just 4.4 gm/dL. My attending and I traded dire prophecies with one another after we dropped our patient off in the ICU. Neither of us thought she would live out the night.
Nearly a week later, she remains alive. But all is not well. Her neurological exam remains remarkably poor, and each day further dims the hope that she will experience any sort of meaningful recovery.
To me, that is one of the most difficult parts of medicine: knowing you've done your best, knowing you've done as well as anyone anywhere could do, and still feeling that you've been beaten. All you can do is say a prayer for your patient and hope that you can help the next one.
No comments:
Post a Comment